
What is Cultural Competence?
Cultural competence in healthcare is “the ability to provide care to patients with diverse values, beliefs and behaviours, including tailoring delivery to meet a patient’s social, cultural, and linguistic needs”. Cultural competence is not a technical skill to master; it requires changing how people think about and interact with the world around them. Cultural competence is an ongoing process that includes reflective practice and continuous learning – it is not a technical skill.
Key values for cultural competence:
- Inclusivity
- Respect
- Valuing differences
- Equity
- Commitment
Why is Cultural Competence Important?
Cultural competence among healthcare providers can help to overcome health disparities and provide better patient care. Becoming culturally competent helps reduce health inequities by working on respecting diversity, focusing on cultural factors that can affect health, understanding language barriers and learning about other cultures’ beliefs, attitudes and behaviours.
Some benefits of cultural competence include:
- More effective communication and use of time with patients
- Can facilitate more genuine and transparent communication with patients
- Can increase patient treatment compliance
- Helps to build rapport and trust with a patient
- May positively impact clinical outcomes
There are a handful of theoretical frameworks that aim to explain the spectrum of cultural competence. One such framework expresses four stages of clinical competence:
- Cultural awareness
- Cultural sensitivity
- Cultural humility
- Cultural competency
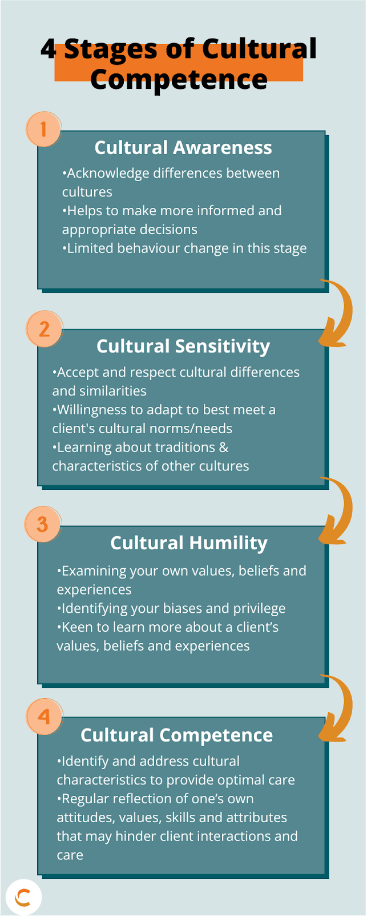
Cultural Awareness
During the awareness stage, differences between cultures are acknowledged and explored.
Cultural Sensitivity
The sensitivity phase occurs when we accept differences between cultures and are willing to adapt to cultural norms to provide patient-centred care. Learning about other cultures’ traditions and characteristics is common in this phase.
Cultural Humility
Asking questions regarding beliefs and values will help to know how culture may impact the recommended interventions. A key component of cultural humility is respecting cultural beliefs and providing individuals with interventions and recommendations that meet their cultural needs. Remember that individuals are the experts of their culture, and cultural identity is individualized.
Cultural Competency
Cultural competence is the final stage and occurs when personal values, beliefs and assumptions are examined to recognize stereotypes, racism or discrimination. Creating a welcoming environment that respects diverse communities and being non-judgemental is important for becoming culturally competent. It is essential to avoid making assumptions and instead get curious. During this stage, cultural preferences are accommodated in a way that doesn’t compromise patient safety.
Achieving cultural competence involves three attitudes:
- Empathy for others
- Curiosity and willingness to ask questions and better understand
- Acknowledgment of the intrinsic value of all humans
Cultural Competency in Eating Disorder Care
Culture is of primary importance in EDC as food often has a strong cultural connection. Foods may have symbolic or spiritual meaning within a culture, which should be considered when providing EDC. Understanding these beliefs and practices will allow for treatment methods and interventions to align with a patient’s personal views and will ensure recommendations are culturally appropriate. Not only should cultural connections to food be considered, but all values and beliefs relating to culture are important considerations when providing EDC. Understanding the barriers, risk factors, and potential outcomes related to culturally competent care can help practitioners provide better EDC. It also helps to increase the likelihood a client adheres to their treatment plan. Common cultural concerns in EDC include racial weight bias, differences in caring for gender-diverse patients and a lack of understanding of Indigenous history and practices.
Barriers, Risk Factors and Potential Outcomes
Barriers to providing culturally competent EDC include:
- Lack of organizational support
- Limited skills to assess differences
- Perceived lack of time
- Limited resources
Diverse groups may experience risk factors for disordered eating. These include food insecurity and disordered eating being used as a coping mechanism which can lead to racially-related weight bias and cultural eating patterns being labelled as disordered.
Racial Weight Bias
Black, Indigenous and People of Colour (BIPOC) may experience disordered eating at a higher weight than white individuals. Stereotypes regarding how an individual living with a restrictive eating disorder “should look” may impact the EDC of BIPOC individuals. It is essential to understand that a person who has not experienced significant weight loss or is not at a low weight can still experience a restrictive eating disorder.
Gender-Diverse Eating Disorder Care
Gender-diverse individuals have elevated rates of disordered eating and often avoid seeking healthcare due to fear of mistreatment. When providing nutrition care to a gender-diverse individual living with an eating disorder, there are a few suggested approaches. These include:
- Using reference values consistent with the sex assigned at birth for patients who have not medically transitioned
- Using reference ranges incorporating both female and male values when sex assigned at birth is not specified
- Recommending treatments and interventions that align with a patient’s medical transition as well as their personal needs
Eating Disorder Care for Indigenous Peoples
Indigenous peoples in Canada continue to experience racism and discrimination when accessing healthcare. One of the main challenges for this population is the lack of culturally appropriate and respectful healthcare. Providing trauma-informed EDC can help to bridge this gap.
Recommended strategies for providing EDC to Indigenous peoples include:
- Learning about the history and everyday lived experiences of Indigenous patients by getting curious and asking questions without making assumptions
- Understanding the effects that high levels of poverty, poor access to goods and services, racism and a loss of identity may have on eating disorders/disordered eating and tailor care accordingly
- Incorporating traditional foods daily can benefit EDC by enhancing nutrition, food security and connection to land and water
- Including a friend or family member in the treatment plan to help provide deeper support
- Encouraging the use of traditional healing practices along with eating disorder treatment or interventions
Trauma-Informed Care
Proving trauma-informed care is a crucial component to becoming culturally competent. For patients who have experienced trauma, the threats in their environment may push eating disorder treatment down their hierarchy of needs and can be a barrier to care. It is important to understand the relationship between food and trauma and how it impacts EDC. Disordered eating can become a coping mechanism for a stressful or unstable environment. Food intake or lack of intake can provide a means of control, which can help the patient gain a sense of comfort. Therefore, proving trauma-informed EDC is essential for BIPOC populations in particular.
The principles for providing trauma-informed EDC include:
- Creating an environment that enhances safety and promotes conversations about race, culture and identity
- Understanding that eating disorders/disordered eating can have intergenerational impacts
- Label structural issues as structural issues
- Understanding and communicating risk appropriately
- Avoid making assumptions and instead get curious about the individual
- Recognize the cultural value(s) of food
A Summary of Strategies for Providing Culturally Safe EDC
- Get curious
- Go beyond culture
- Build rapport with your patients by demonstrating an understanding of food and culture
- Respect that each individual’s knowledge and reality if valuable and valid
- Understand your privilege
- Focus on self-reflection
- Challenge your own beliefs, values, attitudes and assumptions
- Ensure resources, assessment forms, and policies are culturally appropriate for all populations
Our Eating Disorder Care for Health Care Providers online training dives into cultural competence development. If you are interested in learning more, you can register for the training below.
