
The incidence of children younger than 18 who are living with restrictive eating disorders is two times greater than the incidence of type 2 diabetes mellitus in children. So why aren’t primary care providers such as yourself receiving more extensive training in eating disorders?1
The diagnostic (screening) tools used for eating disorder detection vary between healthcare settings.2 This makes eating disorder detection challenging among primary care professionals. As we know, early detection and intervention in eating disorders is incredibly important. It may decrease the risk of long-term pathology as well as disability. In other words, earlier detection means a better recovery.2
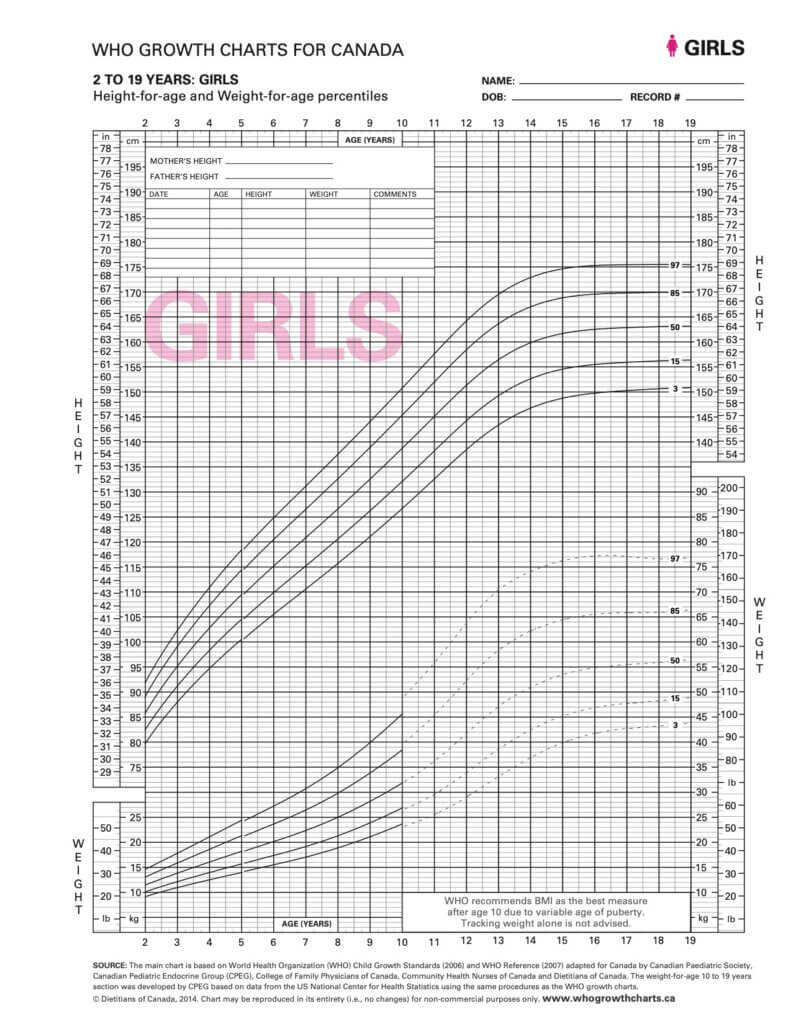
Clinicians should regularly ask their patients about their eating behaviours, body image, and mood to assess their patients’ risk of developing or the presence of an eating disorder.3 Clinicians working with children and adolescents should monitor their patients’ growth charts for any irregularities. An irregularity would be considered a drop of one of greater curves which is grounds for grave concern. This will lead to earlier diagnosis of eating disorders – specifically anorexia nervosa.4 If your patients are children or adolescents, do not use BMI growth charts.3
Pediatricians
Pediatricians play both a crucial and intimate role in the health and development of children and adolescents. Unfortunately, studies continue to indicate that eating disorders in children are often underreported and misdiagnosed by pediatricians. How eating disorders present in children varies depending on the child’s age. The DSM-IV and other diagnostic tools use specific criteria to diagnose eating disorders that may be too strict or narrow to identify early onset eating disorders in children. This makes detection and diagnosis even more challenging. Although eating disorders in young children may present as mild, they can be just as severe as their adolescent counterparts.1
Incidence of Eating Disorder Detection in Pediatrics
The list below details the incidence of restrictive eating disorders in 2011 detected by pediatricians in Canada:
- All children aged 5 to 12 years: 2.6 cases per 100,000 person-years*
- Boys aged 5 to 9 years: 0.4 cases per 100,000 person-years*
- Girls aged 5 to 9 years: 1.3 cases per 100,000 person-years*
- Boys aged 10-12 years: 1.3 cases per 100,000 person-years*
- Girls aged 10-12 years: 9.4 cases per 100,000 person-years*
To summarize, the highest incidence of restrictive eating disorders detected by pediatricians in Canada was in girls between the ages of 10 to 12 years. In contrast, the lowest incidence of restrictive eating disorders was boys between the ages of 5 to 9 years. That is not to say that eating disorders do not occur in young boys.1
*person-years is a measure used in studies determined by the total time individuals participate in the study and the total number of cases over that time period.5
General Practitioners
General Practitioners (GPs) can play a crucial role in the early detection of eating disorders in a primary care setting. Research indicates that individuals living with an eating disorder will consult with their GP more often than those who are not living with an eating disorder. This increased rate in consultation occurs over the five years prior to an individual actually receiving an eating disorder diagnosis.2
Less than one in ten individuals living with bulimia nervosa are diagnosed.2
Unfortunately, GPs often under-detect eating disorders. Less than one in ten individuals living with bulimia nervosa are diagnosed. Similarly, less than half of individuals living with anorexia nervosa are diagnosed. In addition, studies in the UK and Netherlands have found that the detection of eating disorders is 20 percent lower in primary care than it is in the general population.2
The under-detection of eating disorders by GPs in a primary care setting is thought to be because although patients living with eating disorders are visiting their GP more frequently than those without, they are seeing the GP for other clinical reasons.2 That is, they are visiting the doctor for concerns other than eating disorder behaviours.
What can we do as clinicians to change these statistics?
How Eating Disorder Detection Can be Improved
The main way to improve eating disorder detection by primary care providers is education. If primary care providers are better educated on how to identify the presence of an eating disorder, then under detection can be avoided.2 Our team of dietitian nutritionists and therapists at Change Creates Change Eating Disorder Care are passionate about empowering healthcare professionals with the knowledge and tools to detect eating disorders in patients. You’re already doing the work by being here and educating yourself.
There is still a gap in the literature when it comes to eating disorders, especially in children and youth. More studies must be conducted to improve our understanding of eating disorders. Future studies should focus specifically on developing standardized diagnostic (screening) tools, particularly for use in primary care. This will help primary care providers to identify whether their patient is living with an eating disorder.1 The standardized diagnostic (screening) tool should be validated for use in diagnosing the different types of eating disorders outlined in the DSM-5.6
Are You Interested in Learning More?
At Change Creates Change Eating Disorder Care, we strive to educate other healthcare professionals about eating disorders. If you are interested in learning more, you can click below to register for our First, Do No Harm our free webinar for health professionals that will help you navigate what to do if one of your patients is living with an eating disorder.
